


We aren't prepared for the next pandemic
In countries like the UK, it's not even clear what is feasible

It will probably start with a cluster of unusual symptoms. Some of the people with the disease will know each other, but won’t have been exposed to animals, suggesting the infection can spread between people. Then more cases will start appearing in other areas, maybe even in other countries.
The next pandemic could take many forms, but a respiratory infection remains high on the list of probabilities. It could be a new flu virus, or a new coronavirus, or perhaps something else. It might emerge from a market, or a mink farm, or from another source. It may be years away, or months away – or it could be spreading now, yet to be detected.
People often talk about ‘pandemic preparedness’, but increasingly I think this is an unhelpful term. Only in hindsight can we sort events into ‘pandemics’ or ‘outbreaks’ or ‘isolated cases’. In real-time, all these paths begin with a cluster of infections. So if we want to curb pandemics, we need to think about what the response to a small new outbreak will look like.
Post-COVID, there has been a lot of focus on rapid development of diagnostics, treatments and vaccines. The 100 Days Mission aims to have additional tools available within 100 days of a new outbreak, building the success of treatments and vaccines discovered for COVID. Such tools are crucial, but unfortunately, it is less clear what will happen in the meantime. Many groups – including ours – have been working on improving outbreak analytics, so we can understand features like transmission and severity early on. But how will countries respond to a new infection if it turns out to be severe and spreading among humans?
I expect you already have an idea of what some countries will do, given responses to COVID. You may be able to picture events in New Zealand, for example, or Singapore, or South Korea. You can probably imagine what will happen in countries like Sweden too. But what about the UK, or other European countries? Will they reduce transmission with targeted measures like testing and tracing, or introduce blanket measures like limits on social interactions? Will they roll out measures mostly to protect health systems from being overwhelmed, or aim to get infections as low as possible?
Before anyone can choose a strategy, though, there is the more fundamental issue of feasibility. What is even possible for a future response? If we want to be better prepared for the next threat, I think we need to be able to at least answer the (non-exhaustive) questions below.
Could a country like the UK have eliminated COVID, and could it eliminate a flu pandemic?
Some have argued that elimination, if feasible, should be the default option in future for a new severe infectious disease. This would mean local transmission is reduced to zero, with border restrictions keeping out imported cases, alongside strong reactive measures if infections get through and spark a local outbreak.
Although New Zealand is probably the best-known example of COVID elimination, I think countries like Thailand and Vietnam are probably better case studies if arguing in favour of this approach. New Zealand is relatively isolated, so had their first imported case on 28th February 2020 and locked down on 26th March. In contrast, Thailand reported its first case on 13th January and Vietnam on 23rd January. Despite large land borders, both kept infections – and hence deaths – at low levels until well into 2021, after vaccines were available.

It is not hindsight to suggest that elimination could have been debated as an option pre-COVID. Several isolated populations kept out the 1918 influenza pandemic, and researchers in New Zealand even published a cost-effectiveness analysis of a strategy centred on border closures in 2017.
As well as the arguments for elimination, there are also arguments against its feasibility in a country like the UK. First, the UK is highly connected. COVID genomic data suggested that very few imported infections came from China; many came from Italy and Spain, before they reported local outbreaks. There was a similar pattern in later waves, like Omicron, with importations via indirect routes despite ‘red lists’ targeting travel from countries with local outbreaks.

Would it have been feasible – or acceptable – to restrict European travel earlier, in mid-February 2020? This is a question that requires a range of perspectives beyond just epidemiology to debate properly. But it is worth recalling that tourism accounts were posting the below content at the end of February:

Perhaps it wouldn’t be possible to keep infection out initially, but instead it could be driven to zero, then kept out, like in New Zealand and Australia? Ultimately, success here depends on the frequency of introductions and ability to stop local transmission if there is a breakthrough. Analysis of data from New Zealand and Australia estimated around 5 quarantine failures per 100,000 travellers and 6 failures per 1000 positive COVID cases. Between April 2020 and June 2021, there were 37 quarantine failures in these two countries, which resulted in nine lockdowns.
Unless there are extremely few imported infections, combined with extremely effective local measures to stop new outbreaks, a country pursuing an elimination strategy could end up under strict measures for prolonged periods, as happened in Melbourne, which had more time in lockdown that almost anywhere else in the world.
The question of elimination matters because if countries aren’t trying to get infections to zero, then what are they trying to do? Are they trying to keep transmission from growing? Or prevent full hospitals? There will be situations in which elimination isn’t feasible, or the required effort isn’t acceptable. But where - and how - should we draw these lines?
Could travel into a country like the UK be curbed sufficiently in a future public health emergency, given factors like road-based supply chains? Again, this is much bigger than just an epidemiological question. We therefore need to beyond simple statements that elimination ‘obviously’ could work in the UK for a future threat like COVID, or it ‘obviously’ couldn’t work. Instead, we need to understand – and agree on – what is really feasible.
Could targeted measures scale exponentially?
During the West Africa Ebola epidemic in mid-2014, there were many conversations about treatment beds in affected areas, where hospitals were reaching capacity. On one occasion, I remember a plan to double the number of beds in an area in around six weeks’ time. The problem, though, was that Ebola cases were doubling every two weeks. So in six weeks’ time there would likely be eight times as many cases.
When transmission is growing exponentially, it can rapidly outpace resources like hospital capacity, which often scale up in a slower linear manner. I found it frustrating during COVID when too much focus was placed on simply expanding hospital capacity. It would enable more people to be treated, but not all of them. Exponentially rising cases would still overwhelm the health system. In other words, the fundamental problem wasn’t about having more beds; it was about having less transmission.

Unfortunately, reducing transmission can hit a similar resource constraint. Ideally in a disease outbreak, control measures would be directed at where infections are occurring, rather than causing disruption to the wider population (e.g. with blanket lockdowns). But as the number of infections grow, so do the number of contacts people make. On average, people in the UK made around 10 social contacts per day before the COVID pandemic. With hundreds of new cases, there would be thousands of contacts potentially infected.
As well as scale, it also about speed. If we want to use targeted control measures, three key delays drive outbreak dynamics:
A: Delay from a person becoming infectious to start of symptoms.
B: Delay from start of symptoms to isolation of that case.
C: Delay from their infected contacts becoming infectious to quarantine of those contacts.

Isolation of symptomatic cases & contact tracing aims to reduce delays B & C, while screening tests (i.e. rapid tests regardless of symptoms) can reduce delay A & B. There was a lot of focus on tracing 80% of contacts as a performance metric during COVID, but speed is just as important. We need measures that accelerate can get ahead of the epidemic, as well as scale to get on top of it. This will be especially important for a influenza pandemic, where infection happens on a faster timescale than COVID.
If we want a process to scale at speed, we need to consider technological solutions, like digital contact tracing. We know this can scale, given the ‘pingdemic’ in the UK in mid-2021, which was the result of high infection levels, rising social contacts, and an automated contact tracing system doing exactly what it was designed to do. In future, such tracing this also be combined with fast deployment of tests.
This isn’t just hindsight: read about the technological approaches Taiwan had in place in late January 2020. And again, this is about more than epidemiology; it’s about privacy and data infrastructure, as well as social and political acceptability. But the response to COVID shows that some places had thought about this issue much more than others when the first cases started appearing.
Could social inequities be sufficiently addressed?
Testing and tracing alone does nothing to stop an epidemic. What matters is the actions that follow: does a person with a positive test stay away from others? Does a traced – and hence potentially infectious – contact do the same?
Or perhaps a better way to phrase the question: can people do these things? After all, societies are far from equal: insecure jobs made self-isolation – and hence lost income – a huge obstacle for many during COVID. When there was ongoing transmission in Leicester in mid-2020, it led to a local lockdown – and also drew attention to a long-standing issue of worker exploitation.
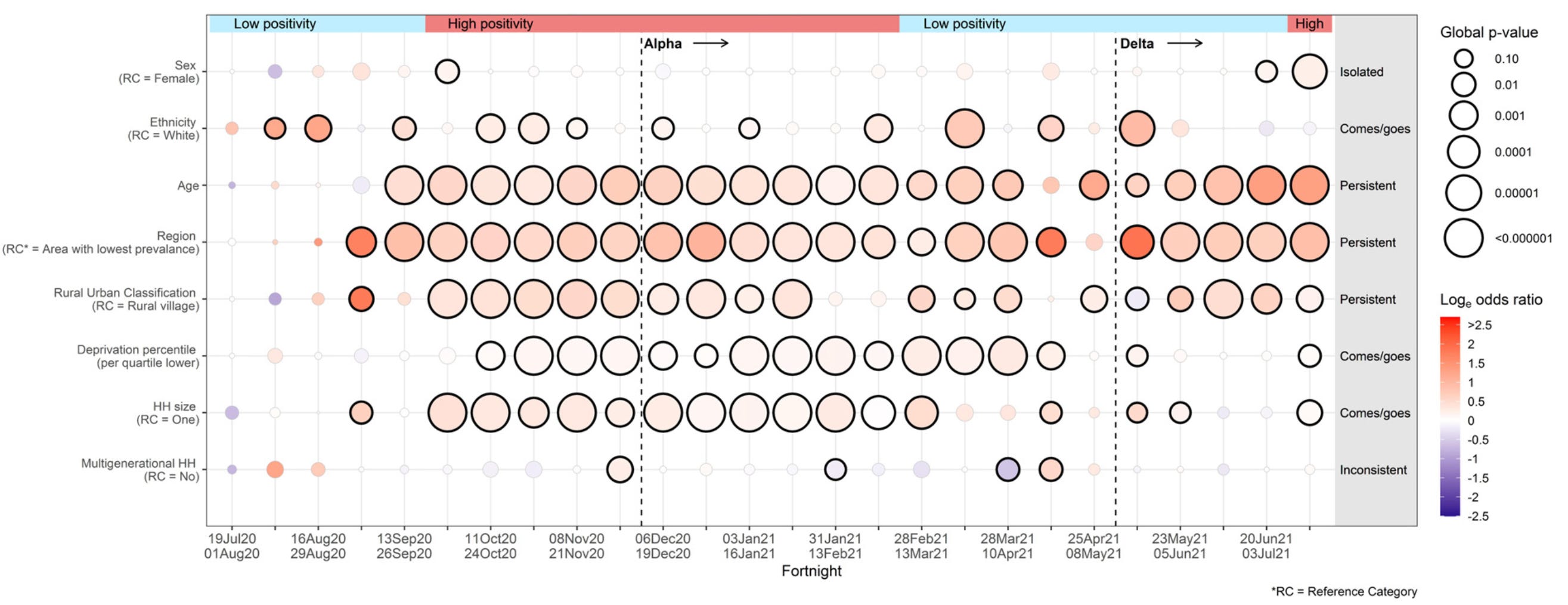
Analysis of the ONS community infection study has illustrated the diversity of factors that influence the risk of catching COVID. In the plot below, darker circles indicate stronger effects and larger circles indicate more evidence for that effect. Ethnicity, age, sex, region, deprivation, household size and composition – there’s evidence that all of these were linked with infection risk.
Many different features of society influence how diseases spread, the impact they have when they do, and the effectiveness of control measures. When it comes to the overall impact of COVID in different countries, we can break these influences down into three main factors:
Long-term population structure & composition (e.g. age, household size, prevalence of pre-existing health conditions).
Pre-pandemic actions (e.g. public health funding, sick leave policy, data laws etc).
Mid-pandemic actions (e.g. timing of social distancing, border closures).
Most of the coverage during COVID – and since – has focused on #3. But to prepare effectively for the next threat, we also need to acknowledge role of #1 (even if we can’t easily change these factors) and #2 (even if complex and less headline friendly). With better sick pay and smaller households, for example, it is easier to slow transmission by getting symptomatic people to self-isolate. People can afford to stay home from work, and won’t infect lots of household members when they do. If we want to curb future outbreaks, we need to understand where the barriers to reducing transmission are, what can feasibly be done about them, and how to deal with trade-offs.
Once again, many of these issues are not new to COVID. There was analysis of the cost-effectiveness of sick leave policies for heath care workers during the 2009 flu pandemic, as well as evaluation of options for future seasonal and pandemic flu waves. The challenges of controlling a respiratory infection were also widely debated during the 1918 flu pandemic. As one 2010 review put it:
Perhaps the most important “lesson” taught by the pandemic was the realization that those measures that worked the best to control a highly infectious disease – bans on public gatherings, school closures, and strict quarantine and isolation – were precisely the ones most difficult to implement in a modern mass society.
…it was exceedingly difficult to get an urban population to stay at home. People needed to work so they could eat; parents wanted their children to go to school; businesses dependent on customers, whether department stores or movie theater operators, did not want to close down.
What could and should be done
On 9th March 2020 – the same day Italy imposed a national lockdown – I watched a talk by Yik-Ying Teo, who was visiting London from Singapore. Before describing the situation in Singapore, and the intensive efforts being made to contain COVID-19, he posed a question: ‘When you see the points I bring up, ask yourself “is this something that my country could or should adopt?”’
In many ways, the question remains. What measures could a country like the UK feasibly adopt if a new influenza virus or coronavirus emerged tomorrow? What measures should it adopt? Until we agree on the answers, I don’t think we can say we’re anywhere near prepared.
Thanks for this!
Two typos I spotted:
"But how will countries respond a new infection"
and "Pindemic" I'm pretty sure was meant to be "Pingdemic"
Great post. Another thought - we have clean water and food, what about enabling clean air? If we improve ventilation in public buildings, offices, apartments (higher filtration, increased air flow) - it would help reduce all respiratory infections. Improvements could start now with all new buildings and renovations required to meet a set (to be decided) ventilation standard.
Reducing air pollution and smoking would also help mitigate the severity of respiratory illness - we are doing this with climate change measures, but probably too slowly.