


What is the best way to stop a pandemic?
The four steps to a disaster, and what we can do about them

Before we start, a quick thank you. My Substack recently hit 2000 subscribers, so thanks so much for signing up, and I hope you’re (still) finding the posts interesting and helpful. As ever, I’d love to hear from people (either in comments on articles or by e-mail) if there’s anything in particular you’d like more of.
Now, on to some epidemiology…
From H5N1 influenza to mpox and Nipah virus, we continue to face the threat of infections that spill over from animals into humans. Although pathogens like rabies don’t spread any further once they get into people (i.e. they effectively have a reproduction number equal to zero), the same isn’t necessarily true of other infections. As we’ve seen with past epidemics such as COVID, Ebola, and pandemic influenza, sometimes infections can get from animals into humans then spread widely, causing enormous damage.
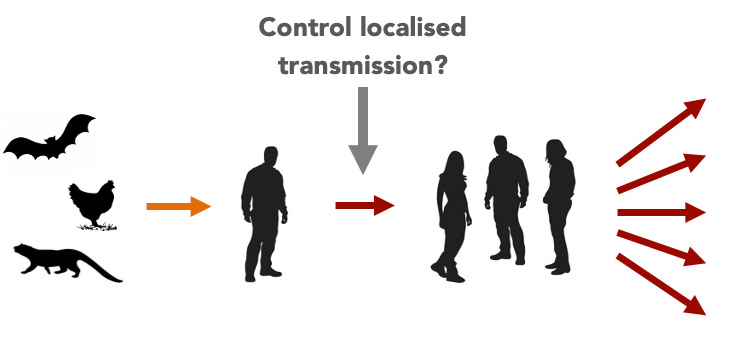
We can break this process of emergence into four main stages, based on the transmission process and species involved:

Which raises the question: where is the best place to intervene to stop a potential pandemic? Let’s run through the four steps in sequence.
Step 1: Target the reservoir
During the 2010s, several groups proposed that pandemics could be tackled by targeting the source, namely the animal reservoirs. These included the Global Virome Project, which aimed to identify potential viral threats before they made the leap into humans. The team noted that would be no small task:
We estimate that discovery of all viral threats and characterization of their risk for spillover, using currently available technologies and protocols, would be extremely costly at over $7 billion. However... the substantial majority of the viral diversity from our target zoonotic reservoirs could be discovered, characterized, and assessed for viral ecology within a 10-year time frame for ~$1.2 billion.
The argument was that such approach, if feasible, could tackle the infection at its source, and hence pre-empt the need for disruptive measures to stop spillover infections or human-to-human transmission. If potential pandemic viruses could be predicted before they emerge into human populations, perhaps it could also inform vaccine development, as well as advancing our scientific understanding of virus diversity and evolution.
But the idea that we can identify pandemic infections before they emerge has a key limitation: predicting virus evolution is hard. A 2017 paper by Jemma Geoghegan and Eddie Holmes made the point that outbreaks are rare compared to vast number of viruses out there, which makes it very difficult to validate any predictions. As they put it:
machine learning requires very large amounts of data to predict common events, whereas studies of disease emergence necessarily use data on rare events to predict rare events.
And even if all viruses currently out there could be sampled and studied, others may evolve in future. After all, knowing about coronaviruses (e.g. SARS, MERS) did not stop SARS-CoV-2 becoming global problem in 2020.
Step 2: Target animal-to-human spillover
If it’s not feasible to target the reservoir, the next step is to target the point at which infections spillover from animals into human populations.

In 2018, a comment piece in Nature re-emphasised the challenges involved in predicting the next pandemic pathogen before it entered human populations. It argued that a better use of resources was to instead spot pathogens promptly as they emerged to become a threat:
We urge those working on infectious disease to focus funds and efforts on a much simpler and more cost-effective way to mitigate outbreaks — proactive, real-time surveillance of human populations.
Take the example of avian influenza H7N9, which first caused outbreaks in humans in early 2013:

In response to these outbreaks, live poultry markets – where humans came into contact with infected birds – were promptly closed. Take the below timeline from early 2013:

In a study of outbreaks during 2013-14, and a more detailed follow up analysis of data from 2013-18, we estimated that closures led to a dramatic reduction in spillover risk1.
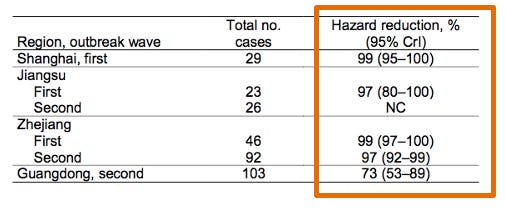
One advantage of intervening as soon as we see evidence of spillover is that if successful, it can be cheaper and less disruptive than dealing with human outbreaks. Evaluating such interventions – like the analysis above – can also help guide better practices to reduce risk for related viruses in future.
However, tackling outbreaks once spillover occurs requires very good surveillance if the virus is already adapted to spread between humans (i.e. larger reproduction number). It may also require large and long-term changes to societies (e.g. widespread market closures) that can be challenging to implement.
Step 3: Control localised outbreaks
When H7N9 caused human infections in 2013-14, there was only a small amount human-to-human transmission; there were a few clusters of spread, often within households, but the reproduction number was below 1.
But the more an infection spreads among human, the more chances it will have to pick up mutations that can help it transmit more efficiently (i.e. an increase in the reproduction number in a susceptible population, given by R0) As a classic paper by Rustom Antia put it:
an increase in R0, even when insufficient to generate an epidemic, nonetheless increases the number of subsequently infected individuals. Here we show that, as a consequence of this, the probability of pathogen evolution to R0 > 1 and subsequent disease emergence can increase markedly.
Indeed, one 2013 study suggested that early clusters of SARS in 2002 had a reproduction number below 1, which subsequently increased by the time it caused major outbreaks in early 2003.
If it’s challenging to predict viruses before they emerge, and detect early spillover events before they spread, perhaps we should focus our efforts on targeting localised transmission, while outbreaks are still small?
This is of course preferable to having a large epidemic, and for pathogens like MERS, SARS and Ebola – which have limited transmission without symptoms – we can make use of targeted measures like isolation and contact tracing in the early stages of an outbreak, alongside some local behaviour change. However, this kind of response requires countries to prepare adequately and answer some tough questions about what they are and aren’t willing to do, particularly for pathogens that are harder to control, as COVID was, and an influenza pandemic would be.
Waiting until a pathogen is already spreading among humans before responding properly also creates the risk that the situation will get much worse, faster.
Step 4: Control widespread epidemics
During the COVID, infections got out of control in many countries, which led to a range of non-pharmaceutical interventions being introduced (e.g. case finding and contact tracing, social distancing, mask wearing, venue closures). However, none of these measures changed the underlying susceptibility in the population. In this situation, ultimately the only way susceptibility changes is either with: 1) the development of pharmaceutical interventions (e.g. vaccines, therapeutics) or 2) the generation of population immunity post-infection.

Once an epidemic is spreading widely, it becomes increasingly difficult to keep infections away from susceptible individuals. This is why suggestions of ‘have a massive epidemic and keep it away from older groups’ during COVID were so absurd: almost 20% of the UK population is over 65.
From Zika to COVID, if countries don’t control – or can’t control – an outbreak early, they’re relying on immunity or treatments to eventually end the epidemic. When mpox spread widely in 2022 – despite in theory being containable through case finding and contact tracing – outbreaks likely ended because of accumulation of immunity alongside behaviour change.
Taking a step back
In the case of H5N1 outbreaks in the US, where five new human cases were reported last week, we are currently at step 2 above. And as we’ve seen, this is often the point at which intervention is both feasible and has a lot of preventative impact for the level of effort exerted. And yet it’s not happening. Poorly understood outbreaks continue in cattle, while human cases continue to emerge (and many more are likely undetected).
With COVID, we didn’t see this early spillover step in real-time; we just saw the situation in early 2020 once we were already at step 3, and rapidly heading into step 4. Fortunately, countries like the US have a head start with H5N1. So they must not waste the advantage and potentially stumble into another pandemic.
Because we had some knowledge of when markets closed, it made it easier to disentangle animal-to-human spillover from local human-to-human transmission. As it happened, we’d later re-use this idea when quantifying the transmissibility of the SARS-CoV-2 in 2021, separating imported cases from abroad (and a known travel ban date) from local transmission.
Adam, thank you for clearly outlining these steps in potential pandemic situation. With covid-19, the impact of human factors in making and accelerating the spread may need to be taken into account in preparing for the next pandemic. Thanks again Adam. This is, as always from you, very thoughtful.
Adam, great article. Great to see a professional, qualified view countering the widespread corporate mainstream media propaganda that "vaccination is the only way out" of a pandemic. When in fact broadly speaking there are three steps that must come before introduction of a novel vaccine/treatment, which by the very rapidity of their development are introduced BEFORE all the usual manufacturer trials, independent studies, meta-analysis of studies, and full regulatory approval processes have been completed, and BEFORE medium to long term health consequences are known, understood and communicated to permit fully informed and therefore legally valid consent of recipients. The risks of ignorance of these health consequences was compounded by widespread employer vaccine mandates, which were unsupported by the science. But Covid-19 vaccine candidate safety is a whole other discussion.
However, why in Step 4 are pharmaceutical interventions and natural immunity post-infection an "either/or" solution?
During Covid, more and more became infected with highly transmissible but milder Delta, then even more highly transmissible Omicron, declared by WHO as a "variant of interest" rather than a "variant of concern" due to its mildness, despite almost overwhelming international pressure brought to bear on the doctor who reported the discovery of this variant to WHO, Dr Sandra Coetzee, head of the South African Medical Association, to exaggerate its severity. Then evidence of viral escape from Delta and rapidly waning immunity to Covid vaccines to as little as zero in as little as 8 weeks emerged globally, in studies from UK, USA, Qatar and Israel. Then near the tail-end of the Omicron wave, evidence emerged - in the form of Covid antibody studies of blood donors in every capital city of Australia, a nation where existed every encouragement to get tested for symptoms, ie free PCR testing, paid "Covid leave" and an effective largely free public medical system - of widespread asymptomatic infection (upwards of 1-in-3 infections), ie the immune system did its job, defeating a pathogen before it replicated to the extent that the body displayed symptoms. Health authorities then spruiked "hybrid immunity" from both vaccination AND natural immunity, accentuating the importance of Covid vaccine derived immunity, and begrudgingly acknowledging natural immunity, if not actively downplaying it.
How they came to this conclusion, I'm not sure. Because the emerging evidence at the time (described above and below, largely ignored by the mainstream corporate media) showed the reverse was true.
I recall the ONLY Covid vaccine manufacturer to publish actual data on antibody response to their vaccine was J & J's one-shot viral vector vaccine, and to be frank the antibody response was - relative to vaccines for other pathogens - underwhelming.
Meanwhile various studies early in the pandemic (and subsequently another 200 or more) highlighted the important role of natural immunity, particularly T-cell memory immunity, which is persistent for decades and responds to highly evolved variants.
I recall two such studies. The first described a "violent and aggresive" T-cell memory immunity response to the original SARS-CoV-2 virus variant in survivors of the 2003 - 2005 SARS pandemic (caused by the virus SARS-CoV), despite a 24% difference in the genetic code between the two viruses, with at least 18 years between exposure. The same study found this T-cell memory immunity also provided a measure of protection against four of the coronaviruses known to cause about a quarter of common colds in humans, despite up to a 50% difference in their genetic code.
Briefly diverging, meanwhile a 0.2% genetic difference expressed in Delta was sufficient to largely defeat Pfizer's mRNA Covid vaccine rendering it only 32% effective, down from the widely publicised "95% effective". Further viral evolution expressed in Omicron was found in the first (South African) study to have rendered it 1/40th as effective against Delta, something CEO & chair Albert Bourla readily publicly admitted, but then urged boosters, claiming it increased immunity by 90%. But wait a minute: 1/40th of 32% is 0.8%, so 90% more effective than 0.8% is... 1.52% effective.
A follow-up study by the authors of the first study found T-cell memory immunity to the SARS-CoV-2 virus in a high proportion of the close household contacts of the Covid-19 sufferers that had expressed no symptoms of infection, highlighting asymptomatic infection and thus effective post-exposure natural immunity response.
Unfortunately, while antibody testing is relatively inexpensive, assessing T-cell memory immunity is not.
I trust that based on the scientific evidence of the relative effectiveness of novel Covid vaccines to a novel & rapidly evolving pandemic pathogen, and history, in future pandemics evidence of infection and apparent recovery, or evidence of antibodies or T-cells to the pathogen of concern, may be considered as an alternative to employer-mandated vaccination with an experimental novel vaccine candidate under emergency use approval, still in its Phase-III trial period, with no data on medium to long term health & safety effects; or in circumstances where evidence of infection and apparent recovery, or evidence of antibodies to the pathogen of concern can be shown, employer vaccine mandates are rulled illegal and unnecessary. Where there is risk, there must be choice.